Dr. Pravin N. Lambade1![]() , Dr. Gunjan K. Hiware2
, Dr. Gunjan K. Hiware2![]() , Dr. Abhijeet
, Dr. Abhijeet
K. Pawar3![]() & Dr. Samruddhi B. Hatwar4
& Dr. Samruddhi B. Hatwar4![]()
1Academic Qualification: Professor, M.D.S Affiliation: Oral and Maxillofacial Surgery
Dr. Rajesh R. Kambe Dental College and Hospital, Akola, Maharashtra 444401 India
2Academic Qualification: M.D.S Affiliation: Oral and Maxillofacial Surgery
Dr. Rajesh R. Kambe Dental College and Hospital, Akola Maharashtra 444401 India
3Academic Qualification: M.D.S Affiliation: Oral and Maxillofacial Surgery
Dr. Rajesh R. Kambe Dental College and Hospital, Akola Maharashtra 444401 India
4Academic Qualification: M.D.S Affiliation: Oral and Maxillofacial Surgery
Institute:. Dr. Rajesh R. Kambe Dental College and Hospital, Akola Maharashtra 444401 India
Corresponding Author Email: drpravinlambade@gmail.com
Article Publishing History
Received: 18/06/2025
Accepted After Revision: 25/08/2025
Mucoceles are common benign lesions of the oral cavity, most frequently affecting the lower lip due to trauma or habitual behaviors such as lip biting. They present as painless, dome-shaped swellings that may vary in size and color, and although benign, can cause discomfort or aesthetic concerns. This case series reports five patients, aged 16 to 52 years, all presenting with lower lip mucoceles of varying durations, sizes, and clinical features. Clinical examination revealed soft, fluctuant swellings, with two cases associated with habitual lip biting and two showing intermittent size fluctuations. All patients underwent complete surgical excision under local anesthesia, including removal of the associated minor salivary glands, followed by histopathological confirmation. Follow-up periods ranged from three months to one year, with no recurrences observed. These findings reinforce the role of meticulous surgical excision and elimination of etiological factors in preventing recurrence and ensuring favorable long-term outcomes.
Mucocele; lower lip; minor salivary gland; surgical excision; recurrence
Lambade P. N, Hiware G. K, Pawar A. K, Hatwar S. B. Mucocele of the Lower Lip: A Case Series and Review of Surgical Management. International Journal of Biomedical Research Science (IJBRS). 2025;01(3).
Lambade P. N, Hiware G. K, Pawar A. K, Hatwar S. B. Mucocele of the Lower Lip: A Case Series and Review of Surgical Management. International Journal of Biomedical Research Science (IJBRS). 2025;01(3). Available from: <a href=”https://shorturl.at/rZptY“>https://shorturl.at/rZptY</a>
INTRODUCTION
Mucoceles are common benign lesions of the oral cavity that result from the accumulation of mucus within the connective tissue due to rupture or blockage of the excretory duct of a minor salivary gland [1]. They are typically caused by mechanical trauma, such as lip biting or direct injury, leading to extravasation or retention of mucus.[2] Clinically, mucoceles present as painless, dome-shaped swellings, often with a bluish or translucent hue, and are most frequently located on the lower lip, although they can occur in other areas of the oral mucosa containing minor salivary glands.[1-3] Their size can vary from a few millimeters to several centimeters, and they may fluctuate over time due to repeated rupture and refilling.[2,4] The etiology of mucoceles is multifactorial, with trauma, habitual behaviors, and anatomical predisposition playing key roles.[1-4] While the lesions are benign, they can interfere with oral function, speech, or aesthetics, particularly when large or recurrent.[2-4]
Differential diagnosis includes fibroma, hemangioma, lipoma, and salivary gland neoplasms, underscoring the importance of accurate clinical assessment supported by histopathological confirmation.[5]Management options range from conservative observation, in cases where spontaneous regression is possible, to various surgical interventions, including complete excision with removal of the associated minor salivary gland to minimize recurrence risk.[6] Alternative methods, such as laser excision, cryosurgery, and marsupialization, have also been reported, each with specific advantages and limitations.[7] The present case series describes the clinical presentation, diagnostic considerations, surgical management, and follow-up outcomes of mucoceles in five patients. The objective of the case series is to determine common patterns and emphasize the role of complete excision in preventing recurrence.
Case Presentations:
Figure 1: Case I – A) Lesion on lower lip, B) Incision, C) Excision of lesion, D) Suturing
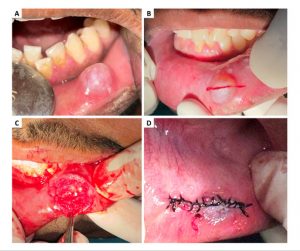
A 24-year-old male presented with a painless swelling of the lower lip of 20–25 days duration (Figure 1). He recalled biting his lower lip about 20 days earlier with subsequent bleeding, after which the lesion gradually enlarged to its present size. There was no history of fever or purulent discharge. Past medical history was non-contributory; he had previously visited a private clinic for the same complaint and received medications. He reported no deleterious habits. On general examination, he was conscious, cooperative, and oriented, afebrile, with pulse 74/min, respirations 16/min, and blood pressure 120/80 mmHg.
Extraorally, the facial profile was straight with competent lips, no gross asymmetry, and no palpable lymphadenopathy. Intraorally, a single round-to-oval, soft, fluctuant swelling measuring approximately 0.5 × 0.5 cm was noted on the inner aspect of the lower lip in the 32–33 region, situated 1–2 mm below the vermilion border and contacting the incisal edges of 22 and 63. Additional findings included mild lower anterior crowding, bilateral Angle Class I molar relation, a missing permanent maxillary left canine, and an over-retained deciduous maxillary left canine (63).
Figure 2: Case II – A) Lesion on lower lip, B) Incision, C) Excision of the lesion,
D) Suturing, E) Excised lesion, F) Pooled areas of mucin (H and E, 4x)

A 52-year-old male presented with a primary complaint of a painless swelling on the inner side of his lower lip on the right side, first noticed three weeks earlier (Figure 2). The swelling had initially been small but gradually increased to its present size. His medical history was non-contributory. The patient reported a habitual lip-biting behavior, and there was no impairment of speech or mastication. Intraoral examination revealed a single, round, soft, and fluctuant swelling located on the inner surface of the lower lip near the region of the right canine.
The lesion was positioned approximately 2–3 mm below the vermilion border and extended downward toward the lingual vestibule, measuring about 6–8 mm in diameter. The overlying mucosa was of the same color as the adjacent tissue, and no other abnormalities were noted in the oral cavity. Based on the clinical presentation and history, a provisional diagnosis of mucocele was considered.
Figure 3: Case III – A) Lesion on lower lip, B) Wound after excision,C) Suturing, D) Excised tissue
A 35-year-old male presented with a complaint of swelling on the lower lip, first noticed approximately three months earlier (Figure 3). The lesion exhibited intermittent changes in size over this period and was not associated with pain. The patient had no relevant medical or systemic history. Clinical examination revealed a soft, painless nodule located on the right side of the labial mucosa. The overlying mucosa appeared normal, and no other intraoral abnormalities were observed. Based on the clinical appearance and history, a provisional diagnosis of mucocele was made.
Figure 4: Case IV – A) Lesion on lower lip, B) Incision over the mucosa, C)
Excision of the lesion, D) Suturing

A 16-year-old male presented with a swelling on the right side of the lower lip, present for about one month, with gradual increase in size over the past three weeks (Figure 4). The lesion was painless, and the patient admitted to habitual lip biting, particularly during periods of concentration. His medical, surgical, dental, and drug histories were unremarkable, and systemic examination—including neurological, musculoskeletal, respiratory, gastrointestinal, and cardiovascular systems—showed no abnormalities. He denied fever, night sweats, fatigue, weight or appetite changes.
Head and neck evaluation revealed no lymphadenopathy, masses, or tenderness, and extraoral assessment showed normal facial symmetry and temporomandibular joint function. Intraorally, a well-circumscribed, soft, dome-shaped swelling measuring approximately 1.5 × 1.5 cm was observed on the right lower labial mucosa adjacent to the occlusal level of teeth 32 and 33. The lesion was mobile, not fixed to underlying structures, and exhibited a bluish hue with a translucent, pearly surface. The overlying mucosa was intact without ulceration or secondary infection. Based on its clinical features and location, a provisional diagnosis of mucocele was made.
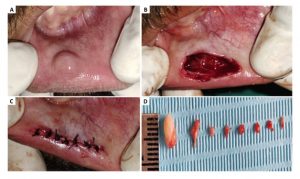
Figure 5: Case V – A) Lesion on lower lip, B) Incision over the mucosa,
C) Excision of the lesion, D) Suturing, E) Healed mucosa

A 23-year-old female presented with a swelling on the lower lip, persisting for the past month (Figure 5). The lesion was soft in consistency, oval in shape, sessile, painless, and demonstrated intermittent variations in size. The patient reported a history of trauma to the lower lip prior to onset. Medical and systemic histories were non-contributory. Intraoral examination revealed a localized swelling on the labial mucosa of the lower lip, with intact overlying mucosa and no signs of ulceration or secondary infection. Based on the clinical features and history, a provisional diagnosis of mucocele was considered.
Management of the cases: In all cases, surgical excision of the lesion was performed under local anesthesia. Following aseptic preparation of the operative site, local infiltration was administered using 2% lignocaine hydrochloride with adrenaline in a 1:80,000 ratio to achieve adequate anesthesia and hemostasis. An elliptical incision was made around the lesion using a No. 15C blade, ensuring inclusion of the overlying mucosa and underlying minor salivary gland tissue. Blunt dissection and stripping with a hemostat were carried out to separate the lesion from surrounding tissues, taking care to avoid rupture of the cystic cavity. The mucocele, along with the associated minor salivary glands, was completely excised to minimize the risk of recurrence.
Flap approximation and primary closure were achieved with simple interrupted sutures using 3-0 silk. Postoperative instructions were provided to all patients, including maintenance of oral hygiene, dietary modifications, and avoidance of lip-biting habits. Appropriate medications, including analgesics and antibiotics, were prescribed. Sutures were removed after one week, and follow-up evaluations were scheduled to monitor healing and assess for any recurrence. The details of all cases, along with the outcomes, are summarized in Table 1.
Table 1. Summary of outcomes of the cases presented in the case series
| Case No. | Age/Sex | Site of Lesion | Treatment Performed | Outcome / Follow-up |
| 1 | 24/M | Inner aspect of lower lip, 32–33 region | Surgical excision under local anesthesia (2% lignocaine with 1:80,000 adrenaline), elliptical incision, blunt dissection, complete removal with associated minor salivary glands, 3-0 silk closure | Uneventful healing, no recurrence at 6-month follow-up |
| 2 | 52/M | Inner surface of lower lip, right canine region | Surgical excision under local anesthesia, elliptical incision, blunt dissection, complete removal with associated minor salivary glands, 3-0 silk closure | Uneventful healing, no recurrence at 6-month follow-up |
| 3 | 35/M | Right side of labial mucosa, lower lip | Surgical excision under local anesthesia, elliptical incision, blunt dissection, complete removal with associated minor salivary glands, 3-0 silk closure | Uneventful healing, no recurrence at 1-year follow-up |
| 4 | 16/M | Right lower labial mucosa, adjacent to teeth 32–33 | Surgical excision under local anesthesia, elliptical incision, blunt dissection, complete removal with associated minor salivary glands, 3-0 silk closure | Uneventful healing, no recurrence at 9-month follow-up |
| 5 | 23/F | Lower lip, labial mucosa | Surgical excision under local anesthesia, elliptical incision, blunt dissection, complete removal with associated minor salivary glands, 3-0 silk closure | Uneventful healing, no recurrence at 3-month follow-up |
DISCUSSION
Mucoceles are among the most frequently encountered benign lesions of the oral cavity, most often affecting the lower lip due to its susceptibility to trauma and the high concentration of minor salivary glands in this region.[1-4] The pathogenesis is generally related to either extravasation of mucus following ductal rupture or retention of saliva due to ductal obstruction.[8] In the present series, all five cases involved the lower lip, consistent with earlier reports highlighting its predilection site. Habitual lip biting was identified in two cases, supporting trauma as a significant etiological factor.[9]
Clinically, mucoceles typically present as painless, fluctuant swellings with a translucent or bluish hue, although deeper lesions may exhibit a normal mucosal color.[10] In our cases, lesion size ranged from 0.5 cm to 1.5 cm, aligning with dimensions reported in previous studies, where mucoceles are generally under 2 cm in diameter. [11] The chronicity varied, with some lesions present for weeks and others persisting for months, and two cases demonstrated intermittent size fluctuations, a feature attributed to periodic rupture and reaccumulation of mucus.[12]
Surgical excision remains the treatment of choice for mucoceles, as it ensures removal of both the lesion and the affected minor salivary glands, reducing the likelihood of recurrence.[13] All cases in this series underwent complete surgical excision using an elliptical incision, with careful dissection to prevent rupture during removal. Histopathological examination in each case confirmed the diagnosis, underscoring its importance in differentiating mucoceles from other swellings such as fibromas, vascular lesions, or salivary gland tumors.
Recurrence is a well-documented concern, particularly if the associated minor salivary glands are not completely excised or if postoperative trauma reinitiates the cycle.[14] No recurrences were noted during follow-up periods ranging from three months to one year in our series, suggesting that meticulous surgical technique and habit modification, such as discouraging lip biting, play a crucial role in long-term success.[15] Alternative treatment modalities, including laser ablation, cryosurgery, and marsupialization, have been reported with varying degrees of success.
Laser excision offers advantages such as reduced intraoperative bleeding and postoperative discomfort, but conventional surgical excision remains a widely preferred approach due to its simplicity, low cost, and predictable outcomes.[7] The present case series reaffirms the clinical characteristics, diagnostic process, and favorable prognosis of mucoceles when managed appropriately. Early recognition, complete excision, and addressing underlying etiological factors are key to preventing recurrence and ensuring optimal patient outcomes.
CONCLUSION
Mucoceles are common, benign lesions of the oral cavity that, while not life-threatening, can cause functional and aesthetic concerns for patients. The present case series highlights their typical occurrence on the lower lip, often associated with mechanical trauma or habitual lip biting, and emphasizes the importance of accurate clinical diagnosis confirmed by histopathological evaluation. Complete surgical excision, including removal of the associated minor salivary glands, proved to be an effective and reliable treatment modality, with no recurrences observed during follow-up. Early detection, elimination of predisposing factors, and meticulous surgical technique are essential to achieving optimal outcomes and preventing recurrence.
Conflict of Interest: There is no Conflict of Interest.
REFERENCES
- Radwan-Oczko M, Sokół I, Babuśka K, Owczarek-Drabińska JE. Prevalence and characteristic of oral mucosa lesions. Symmetry. 2022 Feb 2;14(2):307.
- Swain SK. Oral mucocele: A narrative review. Journal of Indira Gandhi Institute Of Medical Science. 2024 Jul 1;10(2):87-92.
- Ray JG, Bhaje P. Lesions of Oral Mucosa. InIllustrated Pediatric Dentistry-Part 1 2022 Oct 30 (pp. 362-392). Bentham Science Publishers.
- Natarajan E. Benign lumps and bumps. InDental Science for the Medical Professional: An Evidence-Based Approach 2023 Dec 28 (pp. 163-199). Cham: Springer International Publishing.
- Pandarathodiyil AK, Sivapathasundharam B. Diagnostic challenges of superficial mucoceles: An update. Journal of Oral and Maxillofacial Pathology. 2023 Oct 1;27(4):616-21.
- Narendran MR, Balandrar SK, Kannan R. Clinical characteristics, demographic trends, and management outcomes of oral mucoceles: A 10-year retrospective study. Journal of Oral and Maxillofacial Pathology. 2025 Jan 1;29(1):18-23.
- Scribante A, Pellegrini M, Pulicari F, De Martino F, Li Vigni G, Ghizzoni M, Spadari F. Oral cavity mucocele and different surgical treatment strategies: is laser excision effective? A scoping review. Applied Sciences. 2023 Nov 14;13(22):12327.
- Kalaimani G, Sivapathasundharam B, Priyadarshini L, Rajeswari MR, Karthick BP. Mucous extravasation phenomenon: A clinicopathologic evaluation of 68 cases. Journal of Oral and Maxillofacial Pathology. 2024 Apr 1;28(2):182-5.
- Vijayabala GS, Mohanavalli S, Ellampalli H, Janagarathinam VA. Trauma-induced oral mucosal pathologies: A case series. The Saint’s International Dental Journal. 2021 Jul 1;5(2):64-7.
- Philipone E, Yoon AJ, Koutlas IG. Mucosal and Submucosal Lesions. Oral Pathology in the Pediatric Patient: A Clinical Guide to the Diagnosis and Treatment of Mucosal and Submucosal Lesions. 2023 Jul 4:3-115.
- Miranda GG, Chaves-Junior SD, Lopes MP, Rocha TB, Colares DF, Ito FA, Cavalcante IL, Cavalcante RB, Andrade BA, Nonaka CF, Alves PM. Oral mucoceles: A Brazillian multicenter study of 1,901 Cases. Brazilian dental journal. 2022 Oct 21;33:81-90.
- Rongioletti F. New and emerging conditions of acquired cutaneous mucinoses in adults. Journal of the European Academy of Dermatology and Venereology. 2022 Jul;36(7):1016-24.
- Qiuhao WA, Wu Y, Zhang YO, Zhang Z, Xu H, Jiang Y, Luo X. Evaluating the outcomes of minimally invasive therapy vs surgery for oral mucoceles: a systematic review and meta-analysis. Journal of Evidence-Based Dental Practice. 2023 Jun 1;23(2):101841.
- Himelfarb M, Britt MC, Flanagan S, Green MA. What factors influence mucocele recurrence?. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. 2024 May 1;137(5):486-92.
- Wang J, Lin F, Liu Y, Guan X. Effective treatment of multiple oral mucoceles. International Journal of Oral and Maxillofacial Surgery. 2025 Aug 6.


