Department of Prosthodontics, Nair Hospital Dental College, Mumbai, Maharashtra – 400008, India.
Corresponding Author Email: drnaeemabasar@gmail.com
Article Publishing History
Received: 02/07/2025
Accepted After Revision: 25/08/2025
Adult patients frequently seek rapid esthetic correction of anterior spacing yet decline orthodontics. A 24-year-old male presented with midline diastema and generalized maxillary anterior spacing, Angle’s Class III malocclusion, and healthy periodontium (Miller Class I recession). Facially driven planning with diagnostic models and mock-ups established proportional width-to-height targets for space redistribution from canine to canine. Enamel-oriented preparations with supragingival margins were completed, and lithium-disilicate veneers were CAD/CAM fabricated. Adhesive cementation followed hydrofluoric etching and silanization of the intaglio, selective enamel etching, and placement with a light-cure veneer resin to optimize color stability. The restorations achieved space closure, natural emergence profiles, and shade integration; occlusion was refined to stable anterior guidance. Short-term review showed healthy soft tissues with no debonding or marginal discoloration, and the patient reported high satisfaction. This case supports lithium-disilicate veneers as a predictable, minimally invasive alternative when orthodontic treatment is declined.
Lithium disilicate; Porcelain laminate veneers; Diastema closure; Minimally invasive dentistry
Basar N, Kulkarni R, Kharsan V, Bala H. P. Conservative Correction of Midline Diastema and Anterior Spacing with Lithium-Disilicate Veneers: A Case Report. International Journal of Biomedical Research Science (IJBRS). 2025;01(3).
Basar N, Kulkarni R, Kharsan V, Bala H. P. Conservative Correction of Midline Diastema and Anterior Spacing with Lithium-Disilicate Veneers: A Case Report. . International Journal of Biomedical Research Science (IJBRS). 2025;01(3). Available from: <a href=”https://shorturl.at/GFELM“>https://shorturl.at/GFELM</a>
INTRODUCTION
Anterior spacing, midline diastema, and mild proclination are frequent esthetic complaints that can also influence phonetics and anterior guidance.[1] Although orthodontic therapy is the most biologic means of correcting tooth position and space distribution, many adult patients decline comprehensive alignment because of time, cost, or personal preference.[2] Contemporary adhesive dentistry and high-strength glass-ceramics have therefore expanded conservative restorative pathways that can harmonize tooth proportions, close spaces, and improve smile esthetics while preserving the majority of enamel.[3]
Porcelain laminate veneers, particularly lithium disilicate, offer a favourable balance of optical realism and mechanical performance at minimal thicknesses.[4] When preparations remain largely in enamel and margins are kept supra- or equigingival, adhesive durability and periodontal compatibility are enhanced.[5] Predictable bonding rests on meticulous protocols that include hydrofluoric acid conditioning of the ceramic, silanization, selective enamel etching, and the use of light-cure veneer cements to optimize color stability under thin restorations.[6]
Equally critical is facially driven planning. Diagnostic photographs, wax-ups/digital mock-ups, and proportion-based analyses (e.g., width-to-height ratios) guide tooth reduction, contact area placement, and emergence profiles to avoid overbulking during space redistribution. Digital workflows and CAD/CAM fabrication further assist in standardizing contours and interproximal relationships, improving try-in efficiency and shade control.[7]
The present case report outlines a minimally invasive rehabilitation of midline diastema and generalized maxillary anterior spacing in a young adult who declined orthodontics. It details the diagnostic rationale, enamel-oriented preparations, adhesive cementation of lithium-disilicate veneers, and short-term outcomes, emphasizing the principles and clinical steps that support esthetic integration, functional harmony, and patient satisfaction.
Case Presentation: A 24-year-old male presented with the chief concern of an unesthetic smile due to spacing in the maxillary anterior region and requested correction. He reported no relevant medical history and had undergone routine oral prophylaxis six months earlier. General examination revealed an average build and a normal gait.
Clinical findings: Extraoral assessment showed a straight facial profile with an ovoid facial form and competent lips. Temporomandibular joint examination revealed no abnormalities. Intraorally, a midline diastema was present with generalized spacing from right canine to left canine in the maxillary arch (teeth 13–23). Bilateral Angle’s Class III molar relation and canine relationships were recorded. Localised gingival recession consistent with Miller’s Class I was noted without signs of active inflammation. Smile analysis demonstrated that the lip line followed the smile arc, the face was grossly symmetric, and the patient displayed a medium smile line with a premolar-to-premolar natural smile. Micro-esthetic discrepancies were chiefly the midline diastema and the anterior interdental spacing.
Diagnostic assessment: A comprehensive clinical and radiographic evaluation was performed to exclude underlying pathology and confirm suitability for a conservative, enamel-preserving restorative approach aimed at space closure and smile enhancement. The esthetic analysis, occlusal scheme (bilateral Class I), and periodontal status (localized Miller Class I recession) supported a minimally invasive treatment.
Therapeutic options and shared decision-making: Three options were discussed: (1) direct composite buildups, (2) porcelain laminate veneers (laminates), and (3) full-coverage restorations. The comparative advantages, anticipated longevity, tooth-structure preservation, costs, chairside time, reparability, and maintenance were explained. Given the patient’s desire for improved longevity with minimal tooth preparation, lithium-disilicate laminate veneers involving the maxillary anterior teeth were elected. Written informed consent was obtained.
Therapeutic intervention: Shade selection was completed prior to tooth preparation using the VITA 3D-Master shade guide under natural light. Tooth preparation followed a minimally invasive protocol to maintain enamel as the primary bonding substrate. Provisionalization was achieved with a bis-acryl provisional material (OraTemp) to preserve esthetics and function during fabrication (Figure 1).
Figure 1: A) Pre-operative Photograph; B) Gingival retraction after tooth preparation;
C) Digital impression by intraoral scanning; D) Cementation of temporary crowns;
E) Bisque trial (Inset: denture after bisque trial)

At the definitive appointment, provisionals were removed, the field was cleaned, and absolute isolation with a rubber dam was achieved. The definitive ceramic laminates were tried in and evaluated for marginal fit, cervical extension, proximal contacts, and shade integration. The bonding protocol began with conditioning of the restorations: the intaglio surfaces were etched with 9% hydrofluoric acid for 90 seconds, thoroughly rinsed, and air-dried until a uniform frosty appearance was observed. Surface by-products were cleaned by applying 37% phosphoric acid for 60 seconds and rinsing, followed by application of a silane coupling agent for 60 seconds and gentle air-drying. Tooth-side procedures involved selective enamel etching with 37% phosphoric acid for 20 seconds, thorough rinsing, and gentle air-drying to a frosty enamel surface.
A universal adhesive was applied uniformly and gently air-thinned without light-curing to optimize interaction with the luting resin. Each laminate veneer (13 to 23) was luted with a light-cure resin cement (3M™ RelyX™ Veneer Cement). The exclusive use of a light-activated cement was chosen to avoid color shifts associated with chemical initiators in dual-cure agents and because veneer thickness permits reliable photoactivation (Figure 2). After careful seating under controlled pressure, excess cement was removed, and each restoration was light-cured from multiple aspects for adequate polymerization. Occlusion and excursions were verified and adjusted as needed, and margins were finished and polished.
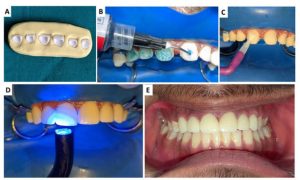
Figure 2: A) Etched prosthesis; B) Etching of teeth; C) Application of bonding agent;
D) Light curing after cementation of veneers; E) Final cemented prosthesis.
Follow-up and outcomes: Immediate postoperative evaluation showed excellent marginal adaptation, appropriate cervical contours, harmonious shade matching, and closure of the diastema and interdental spaces with natural emergence and proportional tooth widths (Figure 3). Soft-tissue response at the margins was healthy with no bleeding on gentle probing. The patient expressed high satisfaction with the esthetic outcome and smile harmony. Postoperative instructions regarding hygiene, avoidance of parafunctional habits, and recall were provided, and the patient was scheduled for periodic reviews.
Figure 3: Comparative demonstration of A) Pre-operative Smile and B) Post-operative Smile

Patient perspective: The patient reported feeling more confident with the appearance of his smile following closure of the anterior spacing and appreciated that the procedure preserved natural tooth structure while delivering a lifelike result.
DISCUSSION
This case illustrates a conservative, patient-centred approach to midline diastema and generalized anterior spacing in a young adult who declined orthodontics. Lithium-disilicate laminate veneers were selected to redistribute spaces, correct tooth proportions, and harmonize the smile while preserving enamel and periodontal health.[8] Comprehensive planning, including diagnostic wax-up/digital mock-up and proportion-guided width-to-height adjustments, enabled controlled space closure without overbulking, maintained a natural smile arc, and respected lip support.[9] Enamel-oriented preparations with supragingival margins, rounded internal angles, and calibrated incisal reduction maximized bond predictability and soft-tissue compatibility, consistent with ultraconservative veneer concepts.[10]
Adhesive protocols were tailored to thin glass-ceramic restorations: hydrofluoric etching of the intaglio, phosphoric-acid cleansing, silanization, selective enamel etching, and rubber-dam isolation to create a stable micro- and chemical bond. [11] A purely light-cured veneer cement supported shade stability and facilitated excess removal through translucent ceramics, aligning with contemporary recommendations for laminate veneer cementation.[10] Material selection balanced optics and strength; lithium disilicate provided lifelike translucency and sufficient flexural performance across multiple anterior units, an approach mirrored in recent esthetic-driven space-management reports that emphasize minimally invasive corrections when orthodontics is refused.[12] CAD/CAM workflow further standardized contours and proximal contacts during space redistribution and has been successfully used in comparable veneer cases to streamline delivery and esthetics.[13]
Functional finishing focused on establishing smooth anterior guidance and eliminating excursive interferences to reduce the risks of marginal chipping and incisal fractures. [14] Early outcomes, including excellent marginal adaptation, stable shade, healthy soft tissue, and high patient satisfaction, are consistent with published experiences when case selection, enamel-based preparation, and meticulous bonding are respected.[12] Limitations include technique sensitivity, susceptibility to parafunctional overload, and the need for patient adherence to maintenance.[15] Nevertheless, for carefully selected patients prioritizing rapid esthetic improvement without orthodontics, lithium-disilicate laminate veneers offer a predictable, minimally invasive solution with favorable short-term performance and a biologically respectful profile. Periodic reviews remain essential to monitor occlusion, margins, and soft tissues and to reinforce protective behaviors.
CONCLUSION
The present case report demonstrates that lithium-disilicate laminate veneers can conservatively correct midline diastema and generalized anterior spacing with excellent short-term esthetics, functional harmony, and soft-tissue health when guided by structured planning and enamel-based adhesive protocols. For patients who decline orthodontics, this minimally invasive approach is a viable alternative; however, long-term success remains contingent on careful case selection, occlusal management, and regular maintenance reviews.
REFERENCES
- Farook TH, Ramees L, Dudley J. Relationship between anterior occlusion, arch dimension, and mandibular movement during speech articulation: A three-dimensional analysis. The Journal of Prosthetic Dentistry. 2025 Mar 1;133(3):881-7.
- Johal A, Damanhuri SH, Colonio-Salazar F. Adult orthodontics, motivations for treatment, choice, and impact of appliances: A qualitative study. American Journal of Orthodontics and Dentofacial Orthopedics. 2024 Jul 1;166(1):36-49.
- FORNA NC, ULEANU R, LUNGU I, DIMOFTE AR. Dental ceramics: advantages and benefits. practice. 2024;4:7.
- JWALITHACLARE M, Arunachalam S, Sneha G, Mondal S. Veneers: A Perfect Solution to Imperfect Teeth. UNIVERSITY JOURNAL OF DENTAL SCIENCES. 2024 Jan 30;10(1).
- GP SC, MS P. EXPLORING THE WORLD OF VENEERS IN CONSERVATIVE DENTISTRY. i-Manager’s Journal of the Indian Dental Association Tamilnadu (JIDAT). 2025 Jun 1;15(2).
- Meyenberg KH. Restorative Gap Management in the Esthetic Zone: Orthodontics| Direct Composite Bonding| Veneers| Bonded & All-Ceramic Bridges| Implants. Quintessenz Verlag; 2023 Apr 24.
- Att W, Witkowski S, Strub JR, editors. Digital workflow in reconstructive dentistry. Quintessenz Verlag; 2021 Feb 1.
- Villalobos-Tinoco J, Floriani F, Rojas-Rueda S, Mekled S, Conner C, Colvert S, Jurado CA. Enhancing Smile Aesthetics and Function with Lithium Disilicate Veneers: A Brief Review and Case Study. Clinics and practice. 2025 Mar 18;15(3):66.
- Talpos S, Titihazan F, Veja I, Dobos M, Rominu M, Negrutiu ML, Sinescu C, Adelina S, Pop DM, Zaharia C, Bolchis V. The Role of Preparation Geometry in Ceramic Veneers: A Comprehensive Literature Review. Medicine in Evolution. 2025 Jun 16;31(2):120-34.
- Morita RK, Hayashida MF, Pupo YM, Berger G, Reggiani RD, Betiol EA. Minimally invasive laminate veneers: clinical aspects in treatment planning and cementation procedures. Case reports in dentistry. 2016;2016(1):1839793.
- Maier E, Bordihn V, Belli R, Taschner M, Petschelt A, Lohbauer U, Zorzin J. New Approaches in Bonding to Glass-Ceramic: Self-Etch Glass-Ceramic Primer and Universal Adhesives. Journal of Adhesive Dentistry. 2019 May 1;21(3).
- Mall V, Gaikwad A, Sachdev SS, Handa A, Chavan S, Kaul M, Gaikwad Sr A. A Minimally Invasive Approach for Correction of Anterior Spacing and Proclination With Lithium Disilicate Glass-Ceramic Veneers: A Case Report. Cureus. 2025 Mar 5;17(3).
- Minase DA, Sathe S, Bhoyar A, Dahihandekar C, Jaiswal T. Porcelain laminate veneers: a case report. Cureus. 2023 Jan 26;15(1).
- Aldowish AF, Alsubaie MN, Alabdulrazzaq SS, Alsaykhan DB, Alamri AK, Alhatem LM, Algoufi JF, Alayed SS, Aljadani SS, Alashjai AM, Alamari AS. Occlusion and its role in the long-term success of dental restorations: a literature review. Cureus. 2024 Nov 7;16(11).
- Alenezi A, Alsweed M, Alsidrani S, Chrcanovic BR. Long-term survival and complication rates of porcelain laminate veneers in clinical studies: a systematic review. Journal of clinical medicine. 2021 Mar 5;10(5):1074.


