Department of Prosthodontics and Crown & Bridge, DY Patil University,
School of Dentistry, Navi Mumbai -400706, India
Corresponding author email: ishitadua12@gmail.com
Article Publishing History
Received: 16/10/2025
Accepted After Revision: 20/12/2025
Rehabilitation of the maxillary anterior esthetic zone becomes particularly challenging when implant-supported crowns must be seamlessly integrated with adjacent natural teeth. This case report describes the comprehensive esthetic rehabilitation of a 27-year-old female with implants in the 11 and 21 regions and disharmonious maxillary anterior alignment. A digitally driven workflow using Digital Smile Design (DSD) and a diagnostic wax-up was employed to establish facially guided tooth proportions and smile harmony. Peri-implant soft tissue was sculpted using temporary abutments and flowable composite to develop a natural emergence profile prior to definitive impressions. Minimally invasive window veneer preparations were performed on adjacent anterior teeth using preparation indices derived from the planned design. A customized open-tray impression captured the conditioned soft-tissue contours, followed by zirconia abutment trial, bisque try-in, and final cementation of implant crowns and lithium disilicate veneers. The final outcome achieved improved smile aesthetics with satisfactory functional integration and high patient satisfaction.
Digital Smile Design; anterior esthetics; peri-implant soft tissue sculpting; zirconia abutment; lithium disilicate veneers.
Mistry G, Puppala P, Parab S, Chitnis A, Chabria A, Ishita Dua I. Digital Smile Design-Guided Anterior Rehabilitation with Implant Crowns and Lithium Disilicate Veneers: A Case Report. International Journal of Biomedical Research Science (IJBRS). 2025;01(3).
Mistry G, Puppala P, Parab S, Chitnis A, Chabria A, Ishita Dua I. Digital Smile Design-Guided Anterior Rehabilitation with Implant Crowns
and Lithium Disilicate Veneers: A Case Report. International Journal of Biomedical Research Science (IJBRS). 2025;01(3). Available from: <a href=”https://shorturl.at/DBexs“>https://shorturl.at/DBexs</a>
INTRODUCTION
Aesthetic rehabilitation of the maxillary anterior region is among the most technique-sensitive procedures in prosthodontics because success depends on seamless integration of tooth form, shade, and surface texture with the surrounding gingival architecture. The complexity increases when implant-supported crowns must be harmonized with adjacent natural teeth, as minor discrepancies in crown proportions, incisal edge position, and peri-implant soft-tissue contours can compromise smile coherence. Therefore, a facially driven plan that can be predictably transferred from diagnosis to execution is essential.
Digital Smile Design (DSD) provides a structured workflow using standardized extraoral and intraoral photographs and reference lines to improve diagnostic visualization, enhance clinician–technician–patient communication, and translate esthetic objectives into a diagnostic wax-up and guided clinical procedures [1]. Peri-implant soft-tissue management is equally critical for developing a natural emergence profile and symmetry; customized provisional restorations and impression strategies have been advocated to accurately transfer sculpted soft-tissue contours to the definitive cast.[2]. Zirconia abutments are frequently selected in the anterior region for favorable optical outcomes [3], while lithium disilicate veneers provide a conservative, highly esthetic option for adjacent teeth.
This case report presents an integrated, minimally invasive workflow combining DSD, soft-tissue sculpting, zirconia abutments, and lithium disilicate veneers for predictable anterior smile rehabilitation.
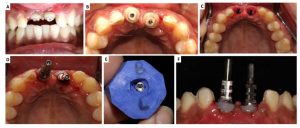
Figure 1: Preoperative Extraoral View – A) Smile and B) Intercuspation; Preoperative Extraoral View – C) Smile and D) Intercuspation

Figure 2: A) Diagnostic Facebow Recording; B) Shade Matching and Shade Selection; C) Digital Waxup Done; D) 3D Printed Model of the waxup; E) Labial View Showing Veneer (Window) Preparation and Putty Index.

Case Report: A 27-year-old female patient presented with a chief concern of an unaesthetic smile and requested definitive prosthetic rehabilitation for implants placed in the maxillary anterior region. She reported dissatisfaction with the overall appearance of her upper front teeth and sought an outcome that would appear natural and harmonious with her facial features. There was no relevant medical history affecting treatment planning, and the patient’s primary expectation was improvement in anterior smile aesthetics with stable function.
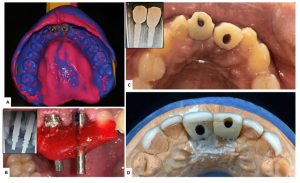
Figure 3: A) and B) Soft Tissue Sculpting Done Using Temporary Abutments and Flowable Composite; C) Intraoral View Showing Anatomic Tissue Sculpting; D) Tissue Sculpting Being Transferred using A Putty Index and Flowable Composite; E) Open Tray Impression Post used to Record the Esthetic Soft Tissue Contour using Flowable Composite.
On clinical examination, endosseous implants were present in the maxillary central incisor regions (11 and 21). The adjacent maxillary anterior dentition exhibited disharmony in alignment and did not follow a pleasing arch form, resulting in compromised smile symmetry. The peri-implant soft tissue contours were also inadequate for an ideal emergence profile, necessitating tissue conditioning before definitive prosthesis. Based on the esthetic demands and the combination of implant-supported and tooth-supported restorations within the smile zone, an interdisciplinary, digitally guided plan was finalized that included Digital Smile Designing (DSD), implant-supported crowns for 11 and 21, and conservative ceramic veneers for the adjacent anterior teeth.
Figure 4: A) Final Impression Made Using Polyvinyl Siloxane; B) Jig Trial; C) Zirconia Abutment Trial Done; D) Bisque Trial
Preoperative extraoral and intraoral photographs were obtained in rest, smile, and maximum intercuspation to facilitate facial and dental analysis. A DSD protocol was used to evaluate midline, occlusal plane, tooth proportions, and smile arc, followed by a digital wax-up to visualize the proposed outcome and guide restorative contours. The digital wax-up was utilized to fabricate a 3D-printed model, allowing verification of proposed tooth position and morphology and enabling accurate transfer of the planned design to the clinical setting.
To optimize peri-implant soft tissue architecture, soft tissue sculpting was performed using temporary abutments and flowable composite to develop a natural gingival contour and emergence profile around the implant sites. Provisional restorations were fabricated intraorally using a matrix derived from the planned contours and were directly relined to achieve appropriate cervical support, gradual transmucosal transition, and symmetry of the peri-implant tissues. The patient was reviewed to ensure soft tissue stability and the desired gingival architecture before proceeding with definitive restorative steps.
A comprehensive diagnostic work-up was then completed, including a facebow record and shade selection. For the tooth-supported component, minimally invasive window veneer preparations were performed on the indicated adjacent maxillary anterior teeth, respecting enamel preservation principles and maintaining controlled reduction based on the planned contours. Labial, palatal, and sectional indices derived from the wax-up were used to guide preparation depth and maintain uniformity of reduction to support predictable ceramic thickness and esthetics.
For definitive impressions, a customized open-tray impression post was used to accurately record the peri-implant soft tissue contours along with implant positions, using polyvinyl siloxane impression material. This ensured faithful transfer of the conditioned emergence profile to the laboratory phase. Subsequent clinical verification was performed through a jig trial, followed by zirconia abutment trial to confirm fit, soft tissue support, and restorative space. A bisque trial of the definitive restorations was carried out to evaluate marginal adaptation, proximal contacts, phonetics, midline, smile arc, and shade harmony under clinical lighting conditions before final finishing and glazing.
Figure 5: A) Postoperative Extraoral Frontal View; B) Postoperative Intraoral View; C) Postoperative Smile View; D) Intraoral View in Occlusion.

Following confirmation of esthetics and fit, final cementation of the implant-supported crowns and lithium disilicate veneers was completed after meticulous surface conditioning and isolation protocols appropriate for each restoration type. Postoperative evaluation demonstrated improved smile symmetry, natural integration between implant restorations and adjacent veneers, and harmonious gingival contours with a stable emergence profile. The patient reported high satisfaction with both functional comfort and the final esthetic outcome, and postoperative intraoral and extraoral views confirmed coherent integration of the prosthetic components with the surrounding dentition and soft tissues.
DISCUSSION
Rehabilitation of the maxillary anterior region is especially technique-sensitive when implant crowns must blend seamlessly with adjacent natural teeth, because esthetic success is dictated by the combined harmony of tooth form, soft-tissue contours, and smile dynamics. In the present case, the emergence profile and peri-implant soft-tissue symmetry were deliberately developed through provisional-driven contouring before definitive prosthesis fabrication, which aligns with the concept of controlled peri-implant tissue conditioning described in the “dynamic compression” technique [4]. At the same time, long-term esthetic predictability in such combined rehabilitations depends on minimizing restoration-related complications, and veneer failures are frequently linked to factors such as substrate/preparation design, cementation variables, and occlusal risk, highlighting the need for a structured, conservative protocol [5].
Digital Smile Design (DSD) supported a facially driven plan in this case by allowing structured evaluation of midline, tooth proportions, and smile framing, and by improving communication and transferability from planning to execution [6]. Clinical literature has also reported that DSD-based workflows can enhance diagnostic predictability and provide patient-centered visualization of proposed esthetic changes during comprehensive rehabilitation [7].
In the implant component, the decision to establish stable peri-implant contours prior to final impressions is consistent with evidence indicating that immediate implant protocols benefit esthetic outcomes when soft-tissue outline is optimized through appropriate provisionalization [8]. Accurate transfer of the developed transmucosal profile was then prioritized using a customized open-tray approach, consistent with techniques advocating custom impression copings to preserve shaped peri-implant gingival architecture [9].
Material selection further contributed to esthetic integration. Randomized clinical evidence has shown comparable clinical behavior of customized zirconia and titanium abutments supporting single implant crowns in posterior/canine regions at midterm follow-up, supporting zirconia as a viable abutment material when esthetic demands are high [10]. Longer-term follow-up from the same trial has also demonstrated favorable outcomes over five years for zirconia and titanium abutments, reinforcing their clinical reliability when appropriately planned and maintained [11].
For the tooth-supported component, systematic evidence confirms that laminate veneers demonstrate high survival, with fracture/chipping among the more frequent complications, emphasizing careful preparation and occlusal control. A diagnostic mock-up–driven preparation approach has been advocated to preserve enamel and improve bonding predictability in veneer therapy, which is consistent with the minimally invasive strategy used here. Finally, lithium disilicate CAD/CAM veneers have shown excellent short-term clinical performance in large retrospective clinical data, supporting their use where conservative, high-esthetic restorations are indicated.
CONCLUSION
The present case report demonstrates that a digitally guided, facially driven workflow can successfully harmonize implant-supported crowns with adjacent tooth-supported veneers in the maxillary anterior esthetic zone. Strategic peri-implant soft-tissue sculpting and accurate transfer of the developed emergence profile, combined with zirconia abutments and lithium disilicate veneers, enabled a natural and cohesive smile outcome. Overall, integrating digital planning with conservative adhesive and soft-tissue management principles can improve predictability and patient satisfaction in complex anterior rehabilitations.
REFERENCES
- Coachman C, Calamita MA. Digital smile design: A tool for treatment planning and communication in esthetic dentistry. Quintessence Dent Technol. 2012;35:103-111.
- Elian N, Tabourian G, Jalbout ZN, Classi A, Cho SC, Froum S, et al. Accurate transfer of peri-implant soft tissue emergence profile from the provisional crown to the final prosthesis using an emergence profile cast. J Esthet Restor Dent. 2007;19(6):306-315. doi:10.1111/j.1708-8240.2007.00128.x
- Naveau A, Rignon-Bret C, Wulfman C. Zirconia abutments in the anterior region: A systematic review of mechanical and esthetic outcomes. J Prosthet Dent. 2019;121(5):775-781. doi:10.1016/j.prosdent.2018.08.005 Wittneben JG, Buser D, Belser UC, Brägger U. Peri-implant soft tissue conditioning with provisional restorations in the esthetic zone: the dynamic compression technique. Int J Periodontics Restorative Dent. 2013 Jul-Aug;33(4):447-455. doi:10.11607/prd.1268.
- Alghazzawi TF. Clinical survival rate and laboratory failure of dental veneers: a narrative literature review. J Funct Biomater. 2024;15(5):131. doi:10.3390/jfb15050131.
- Alharkan HM. Integrating digital smile design into restorative dentistry: a narrative review of the applications and benefits. Saudi Dent J. 2024;36(4):561-567. doi:10.1016/j.sdentj.2023.12.014.
- Meereis CTW, de Souza GB, Albino LGB, Ogliari FA, Piva E, Lima GS. Digital smile design for computer-assisted esthetic rehabilitation: two-year follow-up. Oper Dent. 2016;41(1):E13-E22. doi:10.2341/14-350-S.
- De Rouck T, Collys K, Wyn I, Cosyn J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin Oral Implants Res. 2009;20(6):566-570. doi:10.1111/j.1600-0501.2008.01674.x.
- Schoenbaum TR, Han TJ. Direct custom implant impression copings for the preservation of the pontic receptor site architecture. J Prosthet Dent. 2012;107(3):203-206. doi:10.1016/S0022-3913(12)60059-6.
- Zembic A, Sailer I, Jung RE, Hämmerle CHF. Randomized-controlled clinical trial of customized zirconia and titanium implant abutments for single-tooth implants in canine and posterior regions: 3-year results. Clin Oral Implants Res. 2009;20(8):802-808. doi:10.1111/j.1600-0501.2009.01717.x.
- Zembic A, Bösch A, Jung RE, Hämmerle CHF, Sailer I. Five-year results of a randomized controlled clinical trial comparing zirconia and titanium abutments supporting single-implant crowns in canine and posterior regions. Clin Oral Implants Res. 2013;24(4):384-390. doi:10.1111/clr.12044.


